Research Article
Comparison of Lung Function of normal and persons with chronic low back pain and its relation with duration and severity of Chronic Low Back Pain

Amit Baruaa1, Monalisa Pattnaik2 and Patitapaban Mohanty3*
1MPT, Swami Vivekanand National Institute of Rehabilitation Training and Research, Olatpur, Bairoi, Cuttack, India
2MPT, Assistant Professor (Physiotherapy), Swami Vivekanand National Institute of Rehabilitation Training and Research, Olatpur, Bairoi, Cuttack, India
3Ph.D, Associate Professor (Physiotherapy), Swami Vivekanand National Institute of Rehabilitation Training and Research, Olatpur, Bairoi, Cuttack, India
*Address for Correspondence: Patitapaban Mohanty, Ph.D, Associate Professor, Physiotherapy), Swami Vivekanand National Institute of Rehabilitation Training and Research, Olatpur, Bairoi, Cuttack, India, Email: [email protected]
Dates: Submitted: 18 September 2017; Approved: 12 October 2017; Published: 13 October 2017
How to cite this article: Baruaa A, Pattnaik M, Mohanty P. Comparison of Lung Function of normal and persons with chronic low back pain and its relation with duration and severity of Chronic Low Back Pain. J Nov Physiother Rehabil. 2017; 1: 137-143.
DOI: 10.29328/journal.jnpr.1001015
Copyright License: © 2017 Baruaa A, et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Keywords: Chronic low back pain; Duration of pain; Severity of pain; Lung function
Abstract
Introduction: Chronic low back pain is one of the most prevalent musculoskeletal disorders. Studies have shown certain relations between physical fitness and chronic low back pain (CLBP) by examine some measures of physical fitness. The aim of study was to measure lung function using winspiro PRO in patient with CLBP versus normal healthy individual, and relation of lung function with duration and intensity of CLBP.
Methodology: The study population is comprised of a total of 120 adult persons. 60 subjects with chronic low back pain (41 male and 19 female) with a mean age of 30.69 years (+4.34) and 60 normal individual (39 male and 21 female) with mean age of 29.00 years (+5.34).
Results:The result of comparison of the respiratory parameter forced vital capacity (FVC), and maximal voluntary ventilation (MVV) of individual with CLBP show a significant difference as compare to the normal healthy population. In unrelated ‘t’ test the patient with CLBP (N=60) of age 30.51(SD±4.33), height 169cm (SD±1.23), weight 57.86(SD±7.73) and body mass index (BMI) 20.46 (SD±2.54) show a significant difference in respiratory parameter FVC ( t=17.244, P=0.000), and MVV ( t=11.048, P=0.000) as compare to the normal healthy persons (N=60) of age 29.79 (SD±5.28), height 170cm (SD±1.13), weight 59.40(SD±6.97) and BMI 21.59 (SD±3.29).In patient group- FVC range is 34.0% to 75.00% (52.85%±9.30). MVV range is 45.0% to 86.80%. (63.11%±12.06)In control group FVC range is 63.90% to 98.83% (83.63%±7.59). MVV range is 63.00% to 98.00% (78.96%±7.86).
Conclusions:The overall result of the study show that there is a significant difference in the respiratory parameter that is FVC (forced vital capacity), and the MVV (maximum voluntary ventilation) in persons with chronic low back pain as compare to the healthy person of same age, height, weight and body mass index (BMI).
Introduction
The World Health Organization (WHO) explains the symptom of low back pain as pain felt in the loin i.e. lumbo-sacral region (ICD-10-M54.5). Low back pain (LBP) is defined as pain that is perceived as arising in the region bounded by the 12th rib and the inferior gluteal folds and may also be associated with or without leg pain [1]. Unlike the muscles of the limbs, the muscles involved in lumbopelvic stability also perform a variety of essential homeostatic functions, such as breathing and continence, in addition to movement and control of the trunk [2-5]. Hodges et al. noted that in chronic low back pain (CLBP) the coordinating function between the transversus abdominis and diaphragm was reduced [2]. Thus, it is also possible that faulty posture and anatomical changes cause the physiological function changes in the body that is starting as adoptive breathing strategy, such adoptive strategies would relax the abdominal musculature more than the necessary on inspiration. The adoptive breathing pattern may result in the more upper chest breathing and less efficient diaphragm activity. The purpose of this study is that as there are various factors which comes in play in the patient of the chronic low back pain like the postural disturbances, pain, weakness of the abdominal muscles, the weakness of the thoracic muscles, weakness of the chest wall muscles and also the important respiratory muscles of respiration that is the diaphragm, there are several other factors also like the duration of the low back pain or the intensity and the functional status of the patient.
Method
Sample size-120 subjects (41 male and 19 female in patient group, and 39 male and 21 female in normal person group), Study design-A Non experimental correlation design. Sample design-The study population is comprised of a total of 120 adult persons table 1. These subjects were recruited from the outpatient department of physiotherapy of Swami Vivekanand National Institute of Rehabilitation Training and Research (SVNIRTAR) based on fulfillment of the inclusion and exclusion criteria. Exclusion criteria - Any respiratory and cardiac disease, Previous history of rib fracture, sprains of costo-chondral, costo-sternal and interchondral joint, Spinal surgery, Thoracic or abdominal surgery, Cognitive alteration with musculoskeletal deformity, Patient on drug therapy which alter spirometry parameters like psychotropic drugs, any tumour.
| Table 1 | |
| subjects with chronic low back pain | Normal subjects |
| 60=(41 male and 19 female) | 60=(39 male and 21 female) |
| mean age 30.51±4.33 years | mean age 29.00+5.34 years |
| Patient with chronic low back pain with or without leg pain, Duration of low back pain>3months, VAS score for low back pain>4 age of 18 to 50 years |
Healthy asymptotic subjects age of 18 to 50 years |
After acceptance of the research proposal by the institute’s ethical committee the chronic low back patient are selected from the Out-patient or in-patient department of physiotherapy after fulfill the inclusion or the exclusion criteria. The normal healthy subjects are selected from the students’ population or also the normal subjects who are visited the hospital along with the other patients. After selecting the patient as well normal healthy individual’s informed written consent was also obtained from each subjects. After explaining the purpose of study, subject underwent through a thorough assessment and a general clinical examination to rule out any gross pulmonary or the heart diseases and nervous system disorders. Each subject was interviewed for the oswestry disability index (ODI) questionnaire and the anthropometrical measurement such as height, weight and body mass index (BMI) were also taken.
Additional questions were asked to reveal the type of the occupation to exclude those patients who worked in any industries or in the polluted area or also to see that whether the subject is a sport person. The lung functions were measured by computerized spirometer winspiro PRO. The subject was asked to sit erect in a silent room and took rest for some time and got relax before the procedure. Each subject was shown a demonstration of the test before actual test was carried out on him/her. First mouthpiece was given and asked to try with, by blowing through it as fast and as hard for as long as possible. The minimum of three readings were recorded of each test performed by every subject and the best of the three are selected having reproducibility and validity of recorded parameters. During the procedure subject was asked to wear a nose clip. The lung function parameters included were forced vital capacity (FVC), and maximal voluntary ventilation (MVV). The actual values of all these parameters of patient group as well as the healthy subjects group were taken.
Visual analog scale (VAS), oswestry disability index (ODI) score and duration of low back pain were recorded for the patients with low back pain. Visual analog scale was used to measure subjective pain intensity. This is a card with an uncaliberated scale ranging from 0-10, on one side (with zero representing the worst pain), and a corresponding 10 cm ruler on the other side (with each cm representing one pain level). It has a pointer, which can be easily moved from one end to the other. It is shown to be valid and sensitive [6,7] and has reasonable degree of reproducibility [8].
Oswestry Disability Index is an effective method for measuring disability in patients with LBA, high degree of severity & different causes. It includes 10 6-point scales. Sum of 10 ODI scores is expressed as a % of maximum scores & if patient fails to complete a section % score is adjusted. 1st section rates the intensity of pain & remaining 9 cover the disabling effect of pain on activities of daily living (ADL’s) [9].
Data analysis
All the data were collected by the examiner and the data were analyzed by using the SPSS version 16. Unrelated‘t’ test was performed to find out the significant difference in the respiratory parameters (FVC & MVV) between the Chronic low back pain (CLBP) patient and the normal healthy persons. To find out the correlation between the respiratory parameters (FVC & MVV) and the CLBP parameters (VAS, ODI score and Duration of CLBP) Pearson’s correlation coefficient were calculated. Linear regression was conducted to further analyze the relation between the respiratory parameter (FVC & MVV) and the CLBP (VAS, ODI score & Duration).
Results
The results of comparison of the respiratory parameter (FVC & MVV) of individual with CLBP show a significant difference as compare to the normal healthy population. In unrelated ‘t’ test the patient with CLBP (N=60) of age 30.51(SD±4.33), height 169cm (SD±1.23), weight 57.86(SD±7.73) and (BMI) 20.46 (SD±2.54) show a significant difference in respiratory parameter FVC t=17.244, P=0.000), and MVV ( t=11.048, P=0.000) as compare to the normal healthy persons (N=60) of age 29.79 (SD±5.28), height 170cm (SD±1.13), weight 59.40(SD±6.97) and BMI 21.59 (SD±3.29). In patient group- FVC range is 34.0% to 75.00% (52.85%±9.30) MVV range is 45.0% to 86.80%. (63.11%±12.06). In control group, FVC range is 63.90% to 98.83% (83.63%±7.59). MVV range is 63.00% to 98.00% (78.96%±7.86).
Forced Vital Capacity (FVC): The FVC show a highly negative correlation with the VAS (Graph 1) of CLBP patient (r =-0.721, p=0.000) at significant level of 0.001 (2-tailed).The FVC show a highly negative correlation with the Duration (Graph 2) of the CLBP. (r=-0.821, p=0.000), at the significant level of the 0.001 (2-tailed). The FVC show a highly negative correlation with the ODI score (Graph 3) of the CLBP Patient. (r=-0.707, p=0.000), at the significant level of the 0.001 (2-tailed).In Regression analysis one unit increase in VAS cause 4.408 unit reduction from the predicted FVC in %. In Regression analysis one unit increase in 1 month of duration causes 0.647 unit reduction from the predicted FVC in %. In Regression analysis one unit increase of ODI score causes 0.360 unit reduction from the predicted FVC in %.
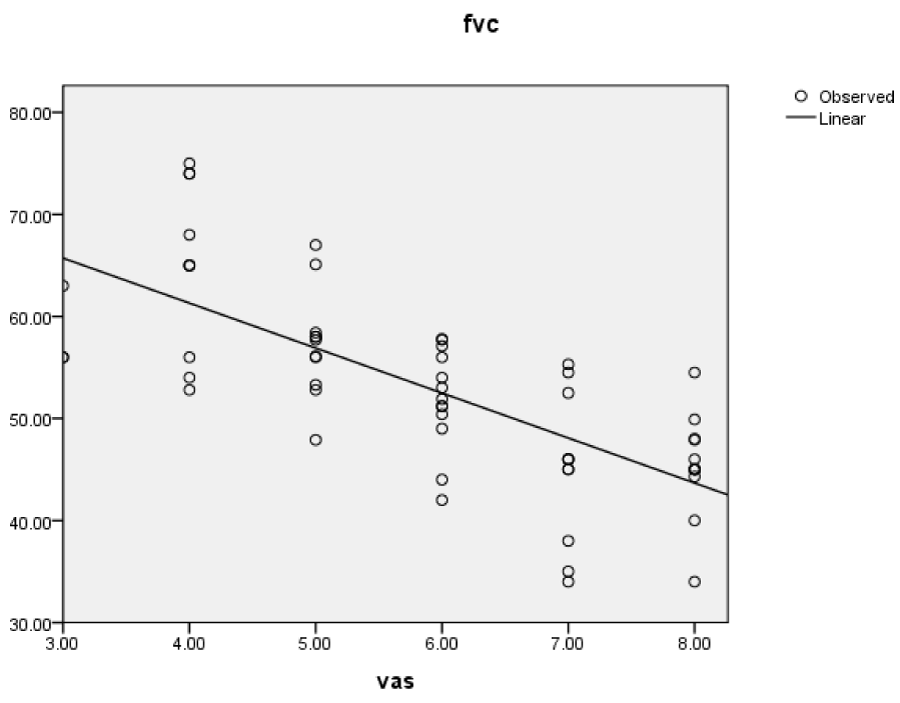
Graph 1: (FVC-VAS)
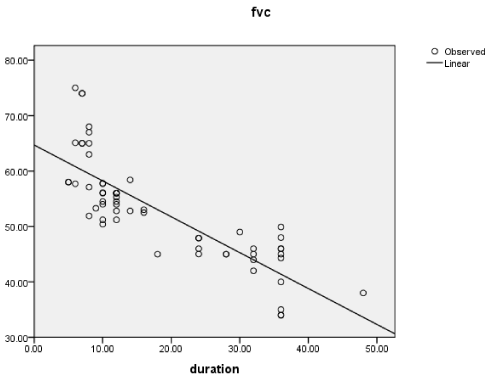
Graph 2: (FVC-DURATION).
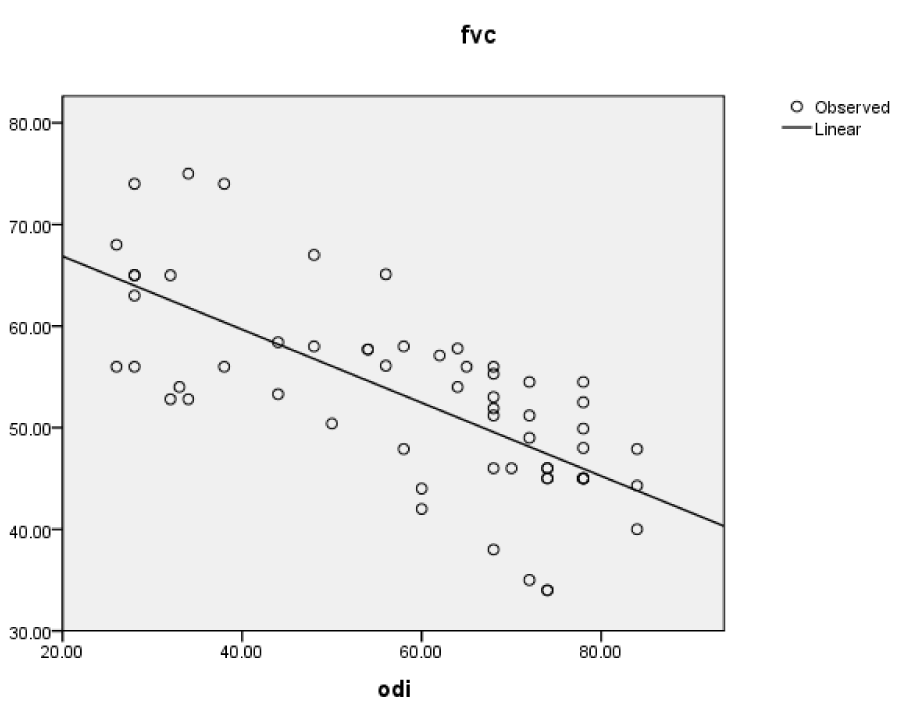
Graph 3: (FVC-ODI).
Maximum voluntary ventilation (MVV): The MVV show a highly negative correlation with the VAS (Graph 4) of CLBP patient (r=-0.828, p=0.000) at significant level of 0.001 (2-tailed). The MVV show a moderate negative correlation with the Duration (Graph 5) of the CLBP (r=-0.640, p=0.000), at the significant level of the 0.001 (2-tailed). The MVV show a highly negative correlation with the ODI score (Graph 6) of the CLBP Patient (r=-0.810, p=0.000), at the significant level of the 0.001 (2-tailed). In the Regression analysis one unit increase in the VAS cause 6.581 unit reduction from the predicted MVV in %. In the Regression analysis one unit increase in the duration of CLBP cause 0.656 unit reduction from the predicted MVV in %. In the Regression analysis one unit increase in the ODI causes 0.537 unit reduction from the predicted MVV in %.

Graph 4:(MVV-VAS).
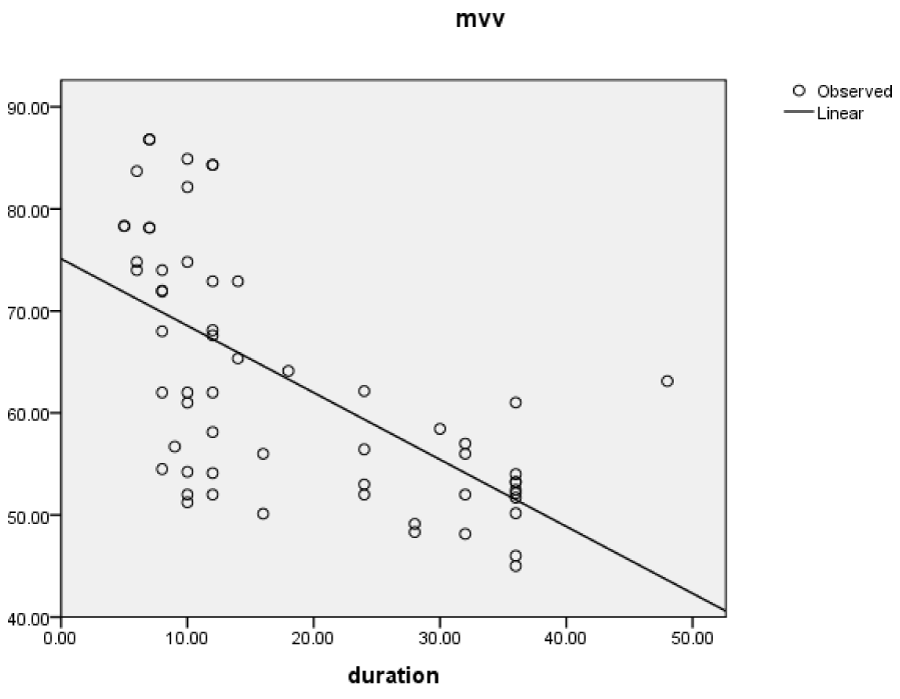
Graph 5: (MVV-DURATION).
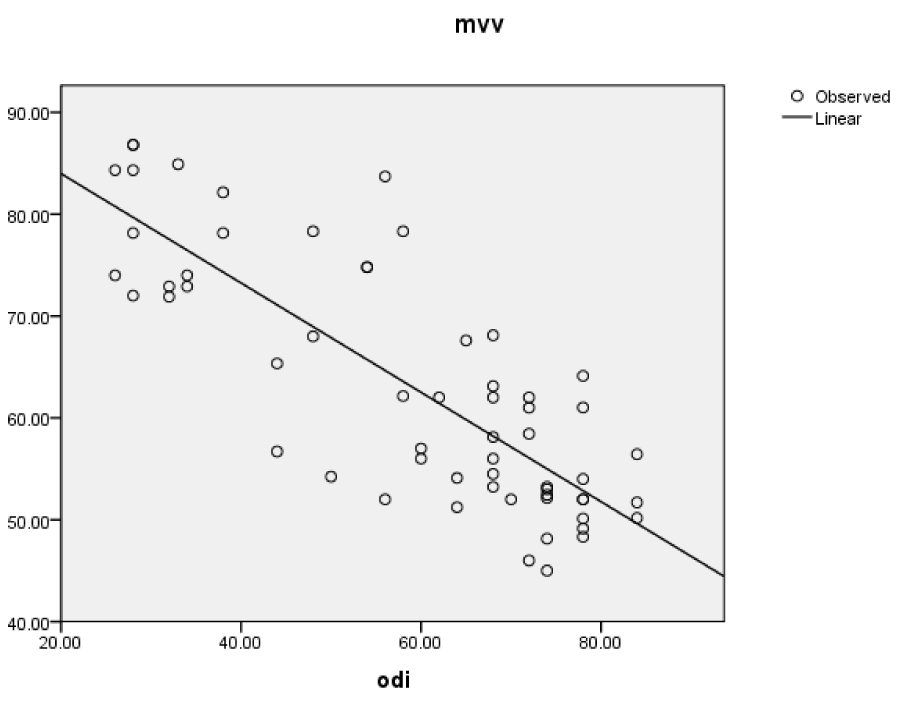
Graph 6: (MVV-ODI).
Discussion
The overall results of the study show that there is a significant difference in the respiratory parameter that is FVC(forced vital capacity), and the MVV(maximum voluntary ventilation) in persons with chronic low back pain as compare to the healthy person of same age, height, weight and BMI. Between the control group and the person with chronic low back pain, the FVC and MVV are significantly reduced (p=0.000) in person with CLBP, as compare to the healthy normal individuals. There is no significant difference in FEV1/FVC ratio (p=0.346) between two group, indicate that the CLBP is more of the restrictive type of lung disorder.
Forced vital capacity (FVC)
The possible explanation for this result may be, due to the reduced chest wall mobility as well as the weakness of the respiratory muscles or the altered recruitment pattern of the respiratory muscles specially the diaphragm and the abdominals. In case of CLBP the chest wall expansion is reduced which is suggested by different studies, the reduced chest wall expansion could be attributed to poor posture due to reduced mobility, manifested by increase thoracic kyphosis or by the slouched posture and this posture lead to the reduction in the rib cage excursion because of possibly altered length tension relationship of the diaphragm. It also has been reported in earlier studies by the Hussain et al. [10] and Gonzalez et al. [11], they suggest that chest wall restriction is the one of the indication of reduced pulmonary function such as FVC, 1 minute forced expiratory volume (FEV1) and the MVV. There are various study which support the hypothesis that is the FVC is reduced in CLBP patient. Pavel Kolar & Alena Kobesova [12], in their study describe that the excursion of the diaphragm is reduced in CLBP patient and the recruitment manner of the diaphragm during inspiration show an altered contraction pattern in CLBP patient as compare to the healthy controls. In their result they show that the FVC of control group is 113.8%±16.0%, and for CLBP patient FVC is 109.7%±12.0%, this result is greatly support the result of this study, as in this study also show the FVC is reduced in patient group as compare to the control group (p=0.000). The abdominal muscles prepare the diaphragm at the end of the expiration for next inspiration, and if the tone of abdominal muscles or the abdominal muscles recruitment is altered the effective deep inspiration get affected it may also be a possible cause for the reduction in the FVC.
Physiotherapy and exercise has long been acknowledged as beneficial for MS symptoms. It facilitates an increase in physical function and independence by improving physical parameters such as muscular power, endurance and reducing fatigue [6-8]. Telerehabilitation is defined as “the use of information and communication technologies as a medium for the provision of rehabilitation services to sites or patients that are at a distance from the provider” [9]. It is considered a form of rehabilitation. Telerehabilitation offers an excellent platform in which to provide necessary physiotherapy interventions to patients who have limited access to transport or inhabit very remote areas [10]. Much of the current literature explores its use in stroke patients (e.g.,[11]), however the rehabilitation method is now being implemented across a broader range of patient groups, including MS [9,12]. To the best of the author’s knowledge, there is no available literature denoting the value of social support in telerehabilitation interventions.
Maximum voluntary ventilation (MVV)
The overall result of this study shows that the MVV is significantly (p=0.000) reduced in patient of CLBP, as compare to the normal healthy persons. The results also suggest that with increase in pain, duration and ODI of CLBP patient, there is more reduction in the MVV. The MVV range is vary in CLBP patient (63.11%±12.06) as compare to the normal healthy persons (78.96±7.86) of same age, weight, height and BMI. The MVV reflect the function of entire ventilatory apparatus and pulmonary function. Presently the MVV test is use as index of maximum voluntary capacity of respiratory system. As the MVV depend on both the pulmonary (lung tissue resistance, thoracic cage movement, respiratory muscles function [13], as well as nonpulmonary factors (motivation, sensorium, muscles force and endurance). These all above factors can affect the MVV in any pathological as well as physiological conditions. The MVV have both the component the inhalation as well as the deep exhalation which required efficient work of respiratory muscles primary as well as the accessory muscles. As in case of CLBP the chest mobility & the respiratory muscles force production get reduced, so it will affect both the component of the MVV.
Conclusion
There was reduction in respiratory parameters (FVC & MVV) in CLBP patient as compared to the normal healthy persons, and also the respiratory parameters get more affected with the severity of CLBP. There was highly significant negative correlation between the pain, duration, and disability of person with CLBP and the respiratory parameters (FVC and MVV).
Limitations
Less control over external variance like temperature, humidity, and diurnal variations. No medical testing was done to rule out any systemic disease it is only based on history and clinical features.
References
- Krismer M, van Tulder M. Low Back Pain Group of the Bone and Joint Health Strategies for Europe Project (2007) Strategies for prevention and management of musculoskeletal conditions. Low back pain (non-specific). Best Pract Res Clin Rheumatol. 2007; 21: 77-91.
- Hodges PW, Gandevia SC. Activation of the human diaphragm during a repetitive postural task. J Physiol. 2000; 522: 165-175. Ref.: https://goo.gl/ihZZm7
- Courtney R. The functions of breathing and its dysfunctions and their relationship to breathing therapy. International Journal Osteopathic Medicine. 2009; 12: 78-85. Ref.: https://goo.gl/BGiQWS
- McGill SM, Grenier S, Bluhm M, Richard P, Susan B, et al. Previous history of LBP with work loss is related to lingering effects in biomechanical physiological, personal, and psychosocial characteristics. Ergonomics. 2003; 46: 731-746. Ref.: https://goo.gl/ZmfCeV
- Sapsford RR, Richardson CA, Maher CF, Hodges PW. Pelvic floor muscle activity in different sitting postures in continent and incontinent women. Arch Phys Med Rehabil. 2008; 89: 1741-1747. Ref.: https://goo.gl/1Tv7Vn
- Murrin KR, Rosen M. Pain measurement. In: Smith G and Govindo BG (editors) Acute pain: London: Butterworth. 1985.
- Kremer E, Atkinson JH, Ignelzi RJ. Measurement of pain: patient preference does not confound pain measurement. Pain. 1981; 10: 241-248. Ref.: https://goo.gl/gUdj6k
- Revill SI, Robinson JO, Rosen M, Hogg MI. The reliability of a linear analogue for evaluating pain. Anaesthesia. 1976; 31: 1191-1198. Ref.: https://goo.gl/mcBhvN
- Vianin M. Psychometric properties and clinical usefulness of the Oswestry Disability Index. J Chiropr Med. 2008; 7: 161-163. Ref.: https://goo.gl/wUa5cZ
- Hussain SN, Rabinovitch B, Macklem PT, Pardy RL. Effects of separate rib cage and abdominal restriction on exercise performance in normal humans. J Appl Physiol. 1985; 58: 2020-2026. Ref.: https://goo.gl/spW8KB
- Gonzalez J, Coast RJ, Lawler JM, Welch HG. A Chest Wall Restrictor to Study Effects on pulmonary Function and Exercise: 2. The Energetics of Restrictive Breathing. Respiration. 1999; 66: 188-194. Ref.: https://goo.gl/QgFrPb
- Frank C, Kobesova A, Kolar P. Dynamic neuromuscular stabilization & sports rehabilitation. Int J Sports Phys Ther. 2013; 8: 62-73. Ref.: https://goo.gl/5wkKSJ
- Neder JA, Andreoni S, Lerario MC, Nery LE. Reference values for lung function tests. II. Maximal respiratory pressures and voluntary ventilation. Braz J Med Biol Res. 1999; 32: 719-727. Ref.: https://goo.gl/Hq9PJe