
More Information
Submitted: 18 July 2020 | Approved: 29 July 2020 | Published: 30 July 2020
How to cite this article: Al Fadani RM, Al Tobaigy IBH, Khan MA. Short term effectiveness of extra corporeal shock wave therapy for plantar fasciitis: A systemic review and meta-analysis. J Nov Physiother Rehabil. 2020; 4: 028-033.
DOI:10.29328/journal.jnpr.1001034
Copyright License: © 2020 Al Fadani RM, et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Keywords: Plantar fasciitis; Pain; Extra corporeal shockwave therapy; Visual analog scale; Meta-analysis

Short term effectiveness of extra corporeal shock wave therapy for plantar fasciitis: A systematic review and meta-analysis
Rayan Mohammed Al Fadani, Ibrahim Bin Hamza Al Tobaigy and Mohammed Amjad Khan*
Comprehensive Rehabilitation Centre, Medina Al Munawwarah, Kingdom of Saudi Arabia
*Address for Correspondence: Mohammed Amjad Khan, Comprehensive Rehabilitation Centre, Medina Al Munawwarah, Kingdom of Saudi Arabia, Email: [email protected]
Background: The argument on whether extracorporeal shock-wave therapy (ESWT) is beneficial in short- term intervention in adults with plantar fasciitis. It is important and necessary to conduct a meta-analysis to make a comparatively more reliable and overall assessment of the outcomes of ESWT in the less than 6 months.
Methods: We conducted a systematic review and meta-analysis of randomized control trials from MEDLINE, EMBASE and CINAHL databases from 2000 to 2020. Randomized trials that evaluated extracorporeal shock wave therapy used to treat plantar heel pain were included. Trials comparing an extra corporeal shock wave therapy with control/placebo were considered for inclusion in the review. We independently applied the inclusion and exclusion criteria to each identified randomized controlled trial, extracted data and assessed the methodological quality of each trial.
Results: Four studies involving 645 patients were included. 3 RCTs (n = 605) permitted a pooled estimate of effectiveness based on overall success rate and composite score of visual analogue scales for pain at follow-up 1 (12 weeks). The pooled data showed no significant heterogeneity at the three-month follow-up (p - value of chi-square = 0.61, p = 0.74 and I2 = 0%). The shock wave group had a better success rate than the control group at the three-month follow-up (OR = 2.26, 95% CI = 1.62-3.15, p - < 0.00001). For reduction of pain the pooled data showed no significant heterogeneity (p - value of chi-Square 0.28 and I2 22%). There were significant differences between the ESWT and control groups for all follow-up visits (random-effect model, three trials, MD = 15.14, 95% CI = 13.86 to 16.42, p - < 0.00001 at three-month).
Conclusion: A meta-analysis of data from three randomized-controlled trials that included a total of 605 patients was statistically significant in favor of extracorporeal shock wave therapy at follow-up 1(12 weeks).
Plantar fasciitis is a common foot disorder in which symptoms may become chronic and functionally disabling [1]. About 10% of people experience plantar fasciitis during globally their life, and 20% - 30% of cases have a bilateral involvement [2]. The plantar fascia is a thick fibrous tissue on the bottom of the foot that protects sensitive plantar structures such as nerves, vessels, muscles and tendons, and in addition, it is responsible for maintaining the plantar arch [3]. Plantar fasciitis is usually diagnosed clinically based on the history of morning heel pain made worse with ambulation on hard surfaces and by the physical findings of pain over the medial aspect of the plantar fascia [4]. There is maximal tenderness at the Plantar fascial origin on the medial process of the calcaneal tuberosity, and pain increases with passive stretching of the plantar fascia [5]. A calcaneal spur may be present in 50% of patients with painful heel [6]. The conservative treatment approach for the plantar fasciitis is focused on decreasing the pain and improving the foot function and easy weight bearing with different treatment strategies from prescribing non-steroidal anti-inflammatory drugs to the orthotic support to correct the foot wear and maintain good arch support. Physical therapy, which has a major role in the management of PF, is considered to be a cost- effective option throughout the world, which includes different modalities and prescribing remedial exercises to stretch the tightened fascia and improve joint mobility and function. The results, from such treatment vary considerably and there is no consensus of the opinion on the best method [7,8]. The use of extra corporeal shock wave therapy in alleviation of pain has been widely postulated and advocated by many researchers during the recent years, although the duration/frequency of treatment and beneficial outcomes in these patients still remain uncertain. The first paper reporting favorable results after the application of shock waves for the treatment of painful heel syndrome was published in 1996 [9]. Since then, numerous studies have reported the promising outcome of shock waves in PF. According to recent systemic reviews by Crawford, et al. [10] and Ogden, et al. [11] evidence is accumulating to support the use of ESWT as an effective treatment for heel pain. The results of the Meta-analysis by Ogden, et al. demonstrated that, of various applications of ESWT on musculoskeletal conditions, the use of ESWT for treating plantar fasciitis was most credible [12].
The purpose of this systematic review and meta-analysis was to conduct a rigorous evaluation using a quantitative synthesis of evidence from randomized controlled trials Evaluate the effectiveness of ESWT in short term. Our aim was to determine if ESWT is effective in the treatment of patients with plantar heel pain when compared with a control group at short-term duration.
Literature search
This systematic review and meta-analysis, was performed in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-analyses (pRISMA) guidelines [13,14] (Figure 1).
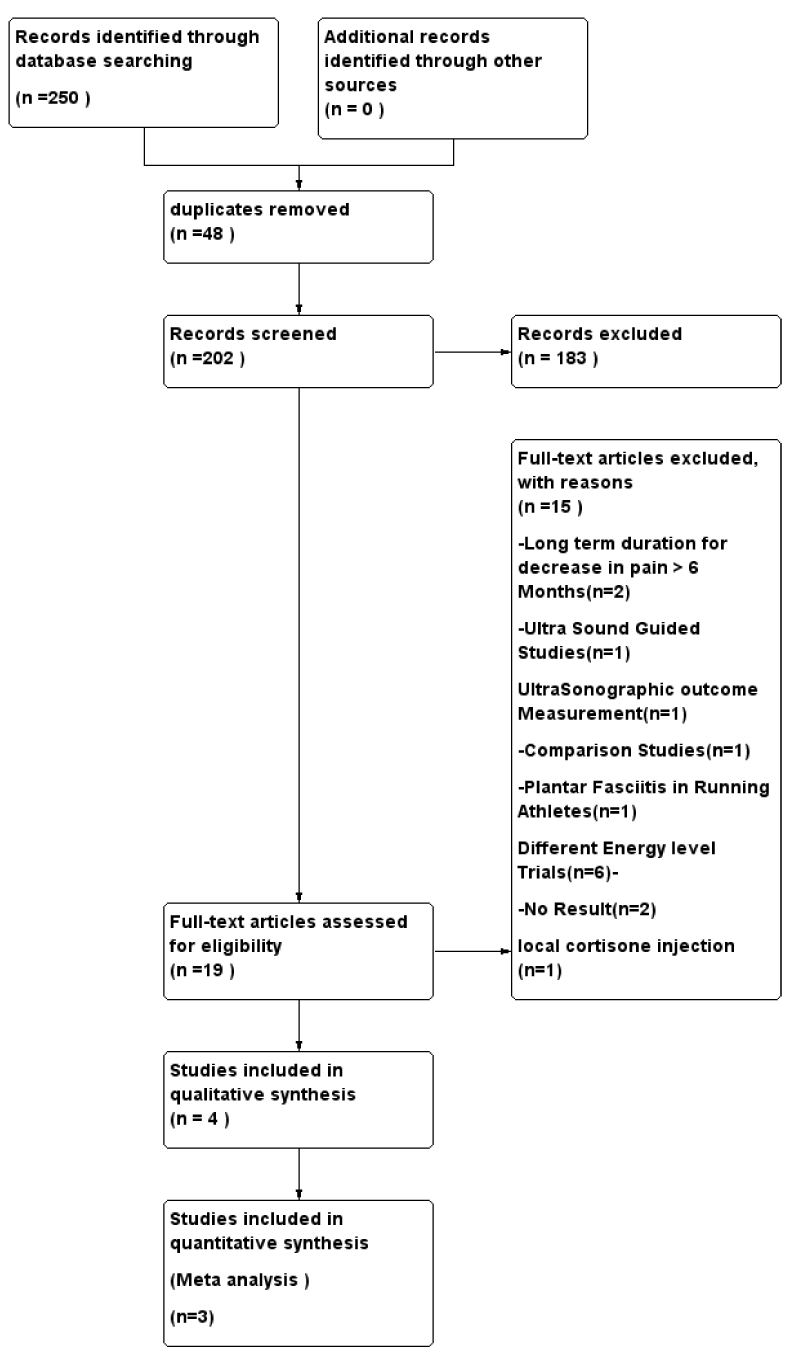
Figure 1: Flow chart of the results of the search strategy.
Search strategy
Using a PICO (p: patients with plantar fasciitis, I: ESWT, C: compared with placebo, O:effective in decreasing the pain in less than 6 months of duration) MEDLINE, Embase and CINAHL database were used to search for relevant literature from the year 2000 to 2020. The text words) «Extracorporeal shockwave therapy or ESWT») AND («Plantar fasciitis» or» heel pain» or «Plantar fasciopathy») AND
(« Randomized controlled trails or RCTs «)
Inclusion and exclusion criteria
Pre-selection criteria of inclusion: Humans, year of publication from 2000 to 2020 full text available in English language: the title and abstracts mentioning the « Extra Corporeal Shock wave Therapy in Plantar fasciitis «randomized, placebo-controlled trials and decrease in pain not more than 6 months after the plantar fasciitis treated with Extra Corporeal shockwave therapy. Non-human trails, case studies/case reports, equipment guided interventions, predefined energy dosage, PF in running Athletes were excluded.
Type of outcomes
The success treatment rate and reduction in the Composite VAS score were the two outcome measures that were adopted to assess the efficacy of ESWTs in our meta-analysis table 1. The definition of successful treatments was varied among articles, such as 60% improvement in pain for at least 2/3 of pain measurements, 60% reduction in morning pain. A previous study has confirmed that 50% decrease of VAS.
| Table 1: Study selection and data extraction. | ||||||||
| Source | SWintensity (mj/mm2) |
Treatment dose | Group | Characteristics of pain for analysis | VAS at Base Line(cm) | VAS after Intervention | Difference in VAS | Use of LA |
| Gerdesmeyer, et al. [17] | 0.16 | 2000 pulses x 3 sessions | RSW Placebo |
Morning pain when taking first steps | 7.5 (1.49) | NA | -4.2 (2.9) | No |
| Gollwitzer, et al. 18] | 0.25 | Total 1.5 mJ/mm2 | FSW Placebo |
Morning pain when taking first steps | 7.5 (1.5) | NA | NA | No |
| Kudo, et al. [3] | 0.64 | Total 3800pulses 2330mJ/mm2 |
FSW Placebo |
Pain during initial walking | 7.5 (1.5) | 3.9 (3.2) | -3.6(2.7) | Yes |
| Moghtaderi, et al. [20] | 0.2 | Total 3000 pulses | ESWT Placebo |
Modified Roles and Maudsley score |
7 ± (1.3) | 3 ± (-0.9) | -4 ± | No |
Score can be defined, as successful pain management [15]. The VAS score is that 50% decrease of VAS score can be defined as successful pain management [15]. The VAS score is widely used to measure a patient’s pain level [16]. The score is self-reported measures of symptoms
Study selection and data extraction
Two reviewers R.M.A and M.A.K completed the same search in the databases and article extraction independently using Rayyan QCRI web App to remove duplicate entries. Published randomized, placebo-controlled trials on the intervention of extra corporeal shock wave therapy for plantar fasciitis fulfilling criteria were included.
The following data was extracted and screened.
Study Identification/Name of the author/type of study/year of publication.
Population/Participants
Diagnosis
Intervention and duration of treatment.
Primary Outcome measures.
Risk of bias in individual studies
Selected studies were evaluated independently for risk of bias assessment using Cochrane risk of bias tool [17] by two authors (R.M.A and M.A.K) to assess the ‘internal validity’. Following the Cochrane risk of bias tool, we assessed the literature for: Selection, Performance, detection,attrition, and reporting bias (Figures 2,3).
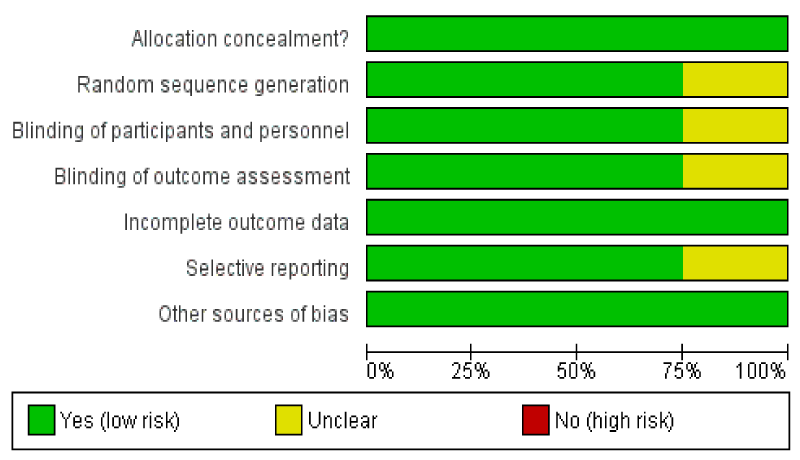
Figure 2: Risk of Bias Summary.
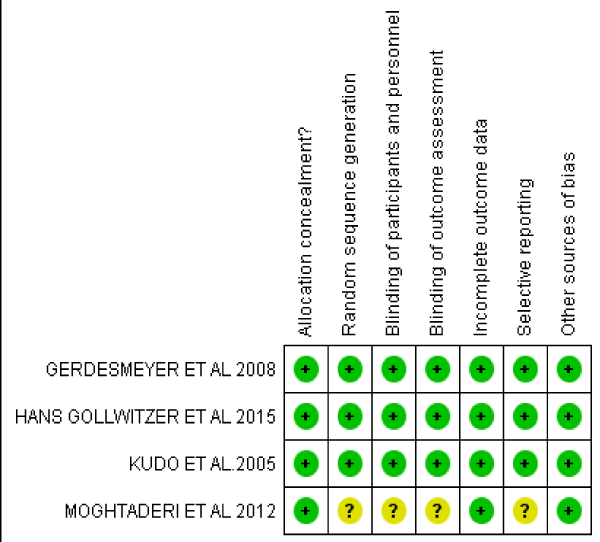
Figure 3: Risk of Bias Summary.
Data synthesis and Statistical analysis.
In the studies by Gerdesmeyer, [18], Gollwitzer, [19] and Kudo, et al. [3], the treatment success rate in ESWT and Placebo Group and the change in composite VAS for 3 months and 12 months was evaluated using meta-analysis. The Meta-analysis and forest plotting were conducted using the Review Manager 5.3 software (Cochrane Collaboration, Oxford, UK). A p-value with smaller than 0.05 was considered significant for all the tests. The effect sizes for outcome measures between ESWT and control/placebo groups for the selected studies were estimated. For Continues data, the effect size was calculated using odds ratio (OR) with 95% CI. Heterogeneity among articles was evaluated using the chi-squared test and I2 statistic, while a p - value of the chi-squared test 0.05 indicated no significant heterogeneity and < 0.05 indicated significance. The I2 statistic was used to evaluate the level of heterogeneity. Heterogeneity was considered low, moderate, high, or very high when I2 was < 25%, 25% – 50%, 50% – 75%, or > 75%, respectively [20].
The study by Moghtaderim, et al. [21] reported the outcome in decreasing the VAS score in plantar fasciitis with the intervention of ESWT on heel and on each trigger point of gastro-soleus muscle. The results were evaluated with the comparison of pain score (100 mm Visual analog Score and modified Roles and Maudsley Score) this study is not considered for meta-analysis and will be analyzed descriptively.
Success rate
The pooled data showed no significant heterogeneity at three-month follow-up (p - value of chi-square = 0.61 p = 0.74 and I2 = 0%). The ESWT group had a better success rate than the control group at three-month follow-up (OR = 2.26, 95% CI = 1.62-3.15, p < 0.00001) (Figure 4a). Pooled data for Heterogeneity from the available results for overall effect for 12 month follow-up showed (p - value of chi-square = 0.03 p = 0.85 and I2 = 0%) with (OR = 2.13, 95% CI = 1.39-3.27, p < 0.0005) Heterogeneity for other sub-group could not be because this only had two article that reported a success rate (Figure 4b).
Figure 4a,b shows Forest plots of treatment success rates in extracorporeal shockwave therapy (ESWT) and placebo-controlled groups at 3-month (a) and 12-month (b) follow-ups.
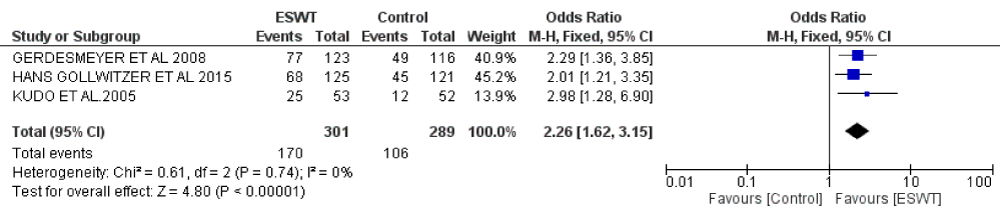
Figure 4a: 3 - month (12 weeks) Follow-up.

Figure 4b: 12 -Month Follow-up.
VAS score
Three (3) included studies reported VAS score to assess the patient’s pain level at 3-month follow up periods. There were 300 in ESWT and 291 placebo-controlled group. The pooled data showed no significant heterogeneity (p value of chi-Square 0.28 and I2 22%). There were significant differences between the ESWT and control groups for all the follow-up visits (random-effect model, three trials, MD = 15.14, 95% CI = 13.86 to 16.42, p < 0.00001 at three-month; for 12 months the pooling data was not possible because of in- sufficient data to assess will be discuss descriptively. The overall effect of one study Z=2.69 (p = 0.007) random-effect model, three trials, MD = 15.40, 95% CI = -4.17 to 26.63, p = 0.38 at 12 months) (Figure 5A,B).
Figure 5 a,b shows Forest plots of visual analog scale (VAS) scores ESWT and placebo-controlled groups at 3-month (a) and 12-month (b) follow-ups.
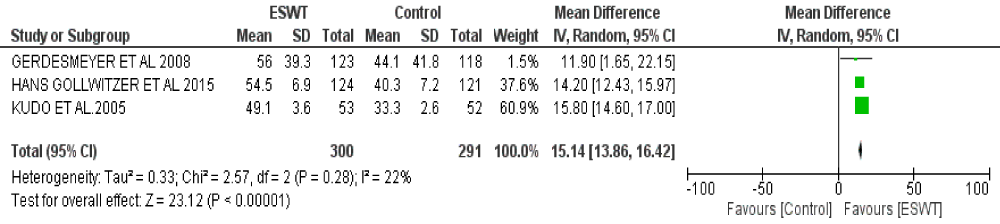
Figure 5a: 3 - month (12 weeks) Follow-up.
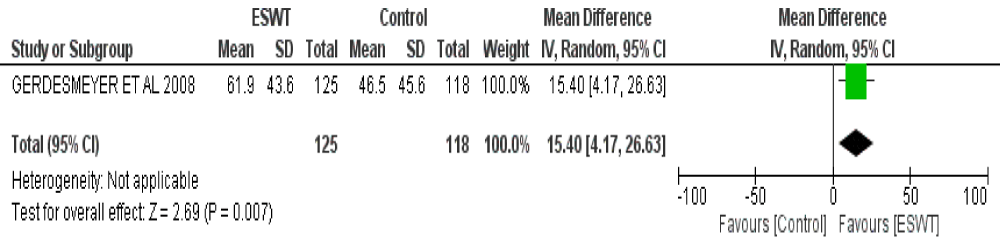
Figure 5b: 3 - month (12 weeks) Follow-up.
Gerdesmeyer, [18] and Gollwitzer, et al. [19] demonstrated the efficacy of ESWT by measuring the percentage change of the VAS composite score twelve weeks after last intervention compared with baseline defined as the sum of three single VAS Scales (1) Heel pain while taking the first step in the morning (2) Heel pain while doing daily activities and (3) heel pain while applying standardized local pressure with the dolor meter and F-Meter respectively. Kudo, et al. [3] Reported the improvement on VAS score from baseline during the first few minutes of walking, Score of none or mild on the pain portion of the AOFAS Ankle-hind foot scale, this study considered deliver the focused ESWT 0.64 mJ/mm2 with the frequency of releasing the shock waves initially at 60 shocks/min at level 1 with increment of 30 shocks/minute at every subsequent level till level 6, reaching approximately 3800 (± 10) shocks/minute at level 7 delivering total energy of 1300 mJ/mm2(ED+) in a single session versus placebo with the administration of medial calcaneal nerve block using 5 ml of 1% xylocaine,15-20 mins prior to the procedure.
ESWT Compared with gastro-soleus trigger points: results of descriptive analysis
Moghtaderi, et al. concluded that combination of ESWT for both plantar fasciitis and gastro-soleus trigger points in treating patients with plantar fasciitis is more effective than utilization it solely for plantar fasciitis [21]. The comparison of visual analog scale score and the modified Roles and Maudsley score had improved groups however, the results were significantly better in the case group compared to control group in mean reduction of score of VAS from 7 ± /-1.3 to 3 ± /0.9 at eight weeks after treatment with p - value < 0.001 in ESWT and p = 0.02 in control group. This reduction was also seen on modified Roles and Maudsley score with p - value < 0.001 ESWT and < 0.01 in Control group.
Identification of eligible studies
The literature search identified 250 publications. 48 duplicate entries were eliminated and 202 articles were selected; 193 of these were excluded after screening their title and abstract. The remaining four (4), involving trials with 645 patients, were evaluated because they met our inclusion criteria.
Study design and population
Table 2 summarized the characteristics of study participants. The included studies were published between 2005 and 2012. All of included studies were RCTs with different follow-up period from 12 week to 12 months. The four (4) studies included a total of 645 patients with Plantar Fasciitis. Three (3) studies including a total of 590 patients who underwent the ESWT (n = 301) and control/placebo (n = 289) treatment for plantar fasciitis. The remaining one (1) study was analyzed descriptively.
| Table 2: Characteristics of the included studies. | ||||||
| Study (design and country) | Number of Patients | Mean age(yrs)* | Intensity (mJ/mm2) | Follow-up | Extracted Outcome Data | Definition of Success |
| Gerdesmeyer, et al. [18] DB, RCT (Germany) | 123 RSW (medium) 116(placebo) | 52.4 52.0 | 0.16 | 3 and 12 months | Success rate | > 60% from baseline at follow-up after treatment for at least 2 of the 3 heel pain (VAS) measurements |
| Gollwitzer, et al. [19] DB, RCT (Germany) | 125FSW (high) 121(placebo) |
50.0 47.4 | 0.25 | 3 months | Success rate | > 60% from baseline at follow-up after treatment for at least 2 of the 3 heel pain (VAS) measurements |
| Kudo, et al. [3] DB, RCT (Canada) | 53 FSW (high) 52(placebo) | 51.1 48.8 | 0.64 | 3 months | Success rate and VAS | > 60% improvement of pain during the first few minutes of walking scored on VAS |
| Moghtaderi, et al. [20] RCT. (Iran) | 20 ESW T(Low) 20(placebo) |
? ? |
0.2 | 8 weeks | Success rate and VAS | Decrement in VAS (p < 0.04) |
Risk of bias within individual studies
The quality assessment of RCTs in the studies was conducted using the Cochrane Risk-of-bias tool, as shown in figures 3,4. The baseline characteristics of all studies were not significantly different between the intervention and the control/placebo groups. In one study [21]. Random sequence generation and allocation, concealment was at high risk and Blinding of outcome assessment was unknown.
Dysfunction in the plantar fascia attributable to any number of primary or secondary causes may lead to acute or chronic heel pain [21]. Patients with undiagnosed heel pain represents as many as 20% of patients presenting to a physician for the diagnosis and treatment of foot problems [22]. Although proximal plantar fasciitis undoubtedly is the most frequent diagnosis of inferior medial heel pain [22]. The optimal non-operative treatment for plantar fasciitis is unclear. Many studies documented good clinical results with different regimens of nonsurgical treatment [23]. Over the years the use of extra corporeal shock wave therapy has been largely accepted to treat wide range of musculoskeletal problems including plantar fasciitis, many RCTs reported the efficacy of ESWT when compared to sham therapy/control group. However, some studies questioned the role of ESWT in acute conditions [24] while some other researchers reported controversies in the effectiveness of different intensity levels of ESWT in plantar fasciitis [25-27]. Many studies reported good results in treating plantar fasciitis with long term intervention of ESWT [27,28]. To our knowledge this is first meta-analysis focusing on effectiveness of ESWT within 6 months post treatment of plantar fasciitis. In our analysis ESWT had favorable results on overall success rate and reduction in VAS score within 6 months of intervention from the baseline. Longer-term follow-up data in two studies were not sufficient or comparable enough for meta-analysis. Gerdesmeyer, et al. [18], Gollwitzer, et al. [19] and Kudo, et al. [3] found success rate > 60% reduction in VAS score at follow-up 1 (12 weeks).The overall success rate showed significant results p < 0.00001 at 12 weeks follow-up as compared with p < 0.0005 at 12 month follow-up. In the study of Gerdesmeyer, et al. [18], reductions in mean VAS composite scores by 44.7% at 12 weeks and 43.2% at 12 months from baseline. Gollwitzer, et al. [19] demonstrated the percentage change of the VAS composite score from baseline increased from -84.0% at the time of follow-up 1(12 weeks) to -96.0% at the time of follow–up 2 in the ESWT group compared with -84.0% at follow-up 1 (12 weeks) to 96.3% at the time of follow-up 2 in the placebo group. Consequently, the outcome shows there was significant improvement at short-term intervention of ESWT in patients with plantar fasciitis.
Ibrahim, et al. [29] concluded the success in the treatment of chronic PF only with two sessions with 2,000 impulses performed 1 week apart. The Mean VAS scores was reduced after ESWT(Radial) from 8.5 ± 0.3 (mean ± SEM) at baseline to 0.6 ± 1.5 at 4 weeks, 1.1 ± 0.3 at 12 weeks and 0.5 ± 0.1 at 24 weeks from baseline [29].
There are some limitations to our study, (1) searched literature was only in English language, (2) only open access literatures were screened and assessed, (3) we focused on the studies which reported the outcome success only in lesser than 6 months of duration from the intervention, whereas many studies demonstrated the efficacy of ESWT in treatment of PF at longer than 6 months also, (4) the types and number of shock waves administered in the included studies were not the same. One trial used radial shock waves whereas two trails used focus shockwaves.
The overall success rate analyzed showed no significant heterogeneity at three-month follow-up. There could be a possibility of reporting bias when interpreting these results due to less number of studies included in the meta-analysis, as there was insufficient comparative data available from the studies for 12-month follow-up.
The main strength of our review include the inclusion criteria of improvement in less than 6 months from the intervention of ESWT in plantar fasciitis. Only RCTs meeting the criteria added to the validity of the statistical results.
We believe that patients with plantar fasciitis can be treated successfully and effectively with ESWT in less than 6 months. More randomized placebo-controlled trials needed to evaluate the efficacy of shockwaves in short term as conservative treatment of plantar fasciitis.
- Theodore GH. Buch M, Amendola A, Bachman C, Fleming LL, et al. Extra Corporeal Shock wave therapy for the Treatment of Plantar Fasciitis. J Foot Ankle Int. 2016; 25: 290-297. PubMed: https://pubmed.ncbi.nlm.nih.gov/15134608/
- Rahbar M, Eslamian F, Toopchizadeh V, Jahanjoo F, Kargar A, et al. A Comparison of the efficacy of Dry needling and Extracorporeal Shockwave Therapy for Plantar Fasciitis: A Randomized Clinical Trial. Iran Red Crescent Med J. 2018.
- Kudo P, Dainty. Clarfield, Coughlin L, Lavoie P, et al. Randomized, Placebo-Controlled, Double-Blind Clinical Trial evaluating the treatment of Plantar Fasciitis with an Extracorporeal Shockwave Therapy Device: A North American Confirmatory Study. J Orthop Res. 2006; 24: 115-123. PubMed: https://pubmed.ncbi.nlm.nih.gov/16435344/
- Fouda KZ. ElLaithy MH., Effect of Low energy versus Medium energy radial shock wave therapy in the treatment of chronic plantar fasciitis. Int J Physiother. 2016; 3: 5-10.
- Buchbiner R, Ptasznik R, Gordon J, Buchanan J, Prabaharan V., et al. Ultrasound-Guided Extracorporeal Shockwave therapy for plantar fasciitis, JAMA. 2002; 288: 1364-1372. PubMed: https://pubmed.ncbi.nlm.nih.gov/12234230
- Lapidus PW. Guidotti FP. Painful heel: Report of 323 patients with 364 painful heels. Clinical orthopedics.1965; 39: 178-186. PubMed: https://pubmed.ncbi.nlm.nih.gov/14289759/
- Gill LH, Kiebzak GM. Outcome of nonsurgical treatment for plantar fasciitis, Foot Ankle Int.1996; 17: 527-532. PubMed: https://pubmed.ncbi.nlm.nih.gov/8886778/
- Wolgin M, Cook Graham C, Mauldin D. Conservative treatment of plantar heel Pain: long- term follow- up, Foot Ankle Int.1994; 15: 97-102. PubMed: https://pubmed.ncbi.nlm.nih.gov/7951946/
- Rompe JD, Hopf C, Nafe B, Burger R. Low-energy Extracorporeal Shockwave therapy for painful heel: A prospective controlled single-blinded study. Arch orthop Trauma Surg. 1996; 115: 75-79. PubMed: https://pubmed.ncbi.nlm.nih.gov/9063856/
- Crawford Atkins D, Edwards J. Interventions for treating plantar heel pain (Cochrane Review). In: Cochrane Library, Issue 4. Oxford, Uk: Updated Software Ltd: 2001. PubMed: https://pubmed.ncbi.nlm.nih.gov/10908473
- Maier M, Steinborn M, Schmitz C, Stäbler A, Köhler S, et al. Extracorporeal Shockwave application for chronic plantar fasciitis associated with heel spur: prediction of outcome by Magnetic resonance imaging Rheumatol. 2000; 27: 2455-2462. PubMed: https://pubmed.ncbi.nlm.nih.gov/11036844/
- Odgen JA, Alvarez RG, Marlow M. Shockwave therapy for Chronic proximal plantar fasciitis: A meta-analysis, foot ankle Int. 2002; 23: 301-308. PubMed: https://pubmed.ncbi.nlm.nih.gov/11991474/
- Moher D, Liberati A, Tetzlaff J, Altman DG, PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement (Chinese edition). J Chin Integr Med. 2009; 6: 889e896 PubMed: https://pubmed.ncbi.nlm.nih.gov/19621072/
- Loke YK, Price A, Herxheimer A. Systematic reviews of adverse effects: framework for a structured approach. BMC Med Res Methodol. 2007; 32. PubMed: https://pubmed.ncbi.nlm.nih.gov/17615054/
- Martin WJJM, Ashton-James CE, Skorpil NE, Heymans MW, Forouzanfar T. What constitutes a clinically important pain reduction in patients after third molar surgery? Pain Res Manag. 2013; 18: 319–322. PubMed: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3917796/
- Hawker GA, Mian S, Kendzerska T, French M. Measures of Adult Pain Visual Analog Scale for Pain (VAS Pain), Numeric Rating Scale for Pain (nRS Pain), McGill Pain Questionnaire (MPQ), Short-Form McGill Pain Questionnaire (SF-MPQ), Chronic Pain Grade Scale (CPGS), Short Form-36 Bodily Pain Scale (SF-36 BPS), and Measure of Intermittent and Constant Osteoarthritis Pain (ICOAP). Arthrit Care Res 2011; 63: S240–S252. PubMed: https://pubmed.ncbi.nlm.nih.gov/22588748/
- Sterne JAC, Savović J, Page MJ, Elbers RG, Blencowe NS, et al. RoB 2: a revised tool for assessing risk of bias in randomized trials. BMJ. 2019; 366: l4898. PubMed: https://pubmed.ncbi.nlm.nih.gov/31462531/
- Gerdesmeyer L, Frey C, Vester J, Maier M, Lowell W, et al. Radial Extracorporeal Shock Wave Therapy is Safe and Effective in the Treatment of Chronic Recalcitrant Plantar Fasciitis: Results of a Confirmatory Randomized Placebo-Controlled Multicenter Study. Am J Sports Med. 36: 2100–2109. PubMed: https://pubmed.ncbi.nlm.nih.gov/18832341/
- Gollwitzer H, Saxena A, DiDomenico LA, Galli L, Bouché RT, et al. Clinically relevant effectiveness of focused extracorporeal shock wave therapy in the treatment of chronic plantar fasciitis: a randomized, controlled multicenter study. J Bone Joint Surg Am. 2015; 97: 701-708. PubMed: https://pubmed.ncbi.nlm.nih.gov/25948515/
- Lou J, Wang S, Liu S, Xing G. Electiveness of Extracorporeal Shock Wave Therapy without Local Anesthesia in Patients with Recalcitrant Plantar Fasciitis: A Meta-Analysis of Randomized Controlled Trials. Am J Phys Med Rehabil. 2017, 96, 529–534. PubMed: https://pubmed.ncbi.nlm.nih.gov/27977431/
- Moghtaderi A, Khosrawi S, Dehghan F. Extracorporeal shock wave therapy of gastroc-soleus trigger points in patients with plantar fasciitis: A randomized, placebo-controlled trial. Adv Biomed Res. 2014; 3: 99. PubMed: https://pubmed.ncbi.nlm.nih.gov/24800188/
- Ogden JA, Alvarez R, Levitt R, Cross GL, Marlow M, et al. Shock wave therapy for chronic proximal plantar fasciitis. 2001; 387: 47-59 PubMed: https://pubmed.ncbi.nlm.nih.gov/11400894/
- Wolgin M, Cook C, Graham C, Mauldin D. Conservative treatment of plantar heel pain: long-term follow-up. Foot Ankle Int. 1994; 15: 97-102. PubMed: https://pubmed.ncbi.nlm.nih.gov/7951946/
- Rompe JD, Furia J, Weil L, Maffulli N. Shock wave therapy for chronic plantar fasciopathy. Br Med Bull. 2007; 81-82: 183-208. PubMed: https://pubmed.ncbi.nlm.nih.gov/17456546
- Speed CA, Nichols D, Wies J, Humphreys H, Richards C, et al. Extracorporeal shock wave therapy for plantar fasciitis. A double blind randomized controlled trial. J Orthop Res. 2003; 21: 937–940. PubMed: https://pubmed.ncbi.nlm.nih.gov/12919884/
- Chang KV, Chen SY, Chen WS, Tu YK, Chen KL, et al. Comparative effectiveness of focused shock wave therapy different intensity levels and radial shock wave therapy for treating of plantar fasciitis: a systemic review and network meta analysis. Arch Phys Med Rehabil. 2012; 93: 1259-1268. PubMed: https://pubmed.ncbi.nlm.nih.gov/22421623
- Ibrahim MI, Donatelli RA, Hellman M, Hussein AZ, Furia JP, et al. Long-Term Results of Radial Extracorporeal Shock Wave Treatment for Chronic Plantar Fasciopathy: A Prospective, Randomized, Placebo-Controlled Trial With Two Years Follow-Up. J Orthop Res. 2017; 35: 1532–1538. PubMed: https://pubmed.ncbi.nlm.nih.gov/27567022/
- Wang CJ, Wang FS, Yang KD, Weng LH, KoWave JY, et al. Treatment for Plantar Fasciitis. Am J Sports Med. 2006; 34: 592-596. PubMed: https://pubmed.ncbi.nlm.nih.gov/16556754/
- Ibrahim MI, Donatelli RA, Schmiz C, Hellman MA, Buxbaum F. Chronic Plantar Fasciitis Treated with Two Sessions of Radial Extracorporeal Shock Wave Therapy. Foot Ankle int. 2010: 31: 391-397. PubMed: https://pubmed.ncbi.nlm.nih.gov/20460065/